You are here:
- Viewpoint - for doctors
Combining surface laser treatment and corneal collagen cross-linking for keratoconus
Treating irregular astigmatism to reverse visual loss in early stage keratoconus
Newer systems for accelerated corneal collagen cross-linking in keratoconus have a homogenous beam profile, and are refractively neutral. Using the Avedro KXL system, and a standard accelerated protocol (7.2mJ/cm2) at Moorfields since 2012, we have not seen the variable, progressive corneal flattening and hyperopic shift that characterized earlier CXL data. This makes it easer to combine CXL with custom surface laser treatment, and we have had some very promising results from a clinical trial of combined treatment using the Schwind Amaris excimer laser platform and ocular wavefront guided transepithelial photorefractive keratectomy (TransPRK). At two years after surgery, patients have significant gains in corrected visual acuity, reduced coma and reduced astigmatism.
Will removing corneal tissue impair the efficacy of CXL? So far, the answer from both our own data and studies elsewhere would appear to be no. Our visual results were stable between one and two years after surgery, and there were no significant changes in corneal shape after the 3-month postoperative examination.
Any risk of destabilising corneal shape should be reduced by removing less tissue, and the Amaris system incorporates a unique instruction set for tissue saving. In essence, we told the laser to correct irregular astigmatism only and not to worry about the resulting sphere or cylinder. This contrasts with earlier combined PRK and CXL treatments in which small optical zones and partial myopic corrections were used. We reasoned that residual sphere and cylinder could easily be corrected with later ICL implantation if required, and avoiding myopic laser correction meant that we could minimize the depth of tissue removal with no compromise to optical zone size or optical quality.
It is important to emphasise that wavefront guided PRK is best suited to fine tuning for irregular astigmatism, rather than gross corneal shape correction; but, based on 2-year results, we are increasingly confident that combined TransPRK/CXL can help patients with early stage visual loss in keratoconus.
I would like to acknowledge Dan Gore, Marcello Leucci, Vijay Anand. Luis Fernandez Vega and the Early Keratoconus Clinic team at Moorfields, and Sam Arba Mosquera and colleagues at Schwind Eye Tech Solutions GmbH for all their hard work on developing our approach to TransPRK/CXL.
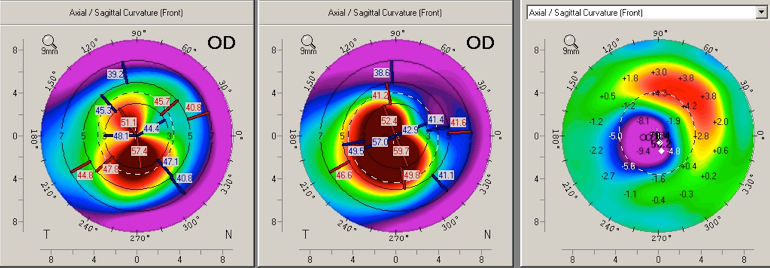
Pentacam subtraction map (left) before (middle) and after (right) TransPRK